早产合并胎膜早破的发生因素及妊娠结局分析
http://www.100md.com
2010年3月25日
 |
| 第1页 |
参见附件(1262KB,2页)。
[摘要] 目的:探讨早产合并胎膜早破的妊娠结局。方法:对本院2007年1月~2008年6月168例确诊为早产合并胎膜早破的产妇资料进行回顾性分析。结果:134例胎膜早破中以流产引产史、感染及胎位不正多见。孕28~34+6周与孕35~36+6周胎膜早破分娩方式比较,差异有统计学意义(P<0.05),新生儿发病率前者明显高于后者(P<0.01)。结论:应进一步重视对胎膜早破的病因,孕前常规妇检,避免多次人工流产和引产,掌握胎膜早破的妊娠相关因素及处理方式,一旦有难产发生,应及时处理,以降低新生儿发病率和死亡率。
[关键词] 早产;胎膜早破;发生原因;妊娠;结局分析
[中图分类号] R714.4 [文献标识码]B [文章编号]1674-4721(2010)03(c)-138-02
Factor in the occurrence of premature rupture of membranes and pregnancy outcome
LI Chenkai
(Gaobu Hospital of Dongguan City,Guangdong Province, Dongguan523260,China)
[Abstract] Objective:To investigate pregnancy outcome of preterm premature rupture of membranes. Methods: The hospital in January 2007 to June 2008 confirmed 168 cases of premature rupture of membranes maternal data were analyzed retrospectively. Results: 134 patients with premature rupture of membranes in the history of abortion, abortion, infection, and malposition more common.28-34+6 week pregnant and pregnant 35-36+6 week PROM mode of delivery, the difference was statistically significant (P<0.05),neonatal morbidity was significantly higher than the former the latter (P<0.01).Conclusion: We should pay greater attention to the cause of premature rupture of membranes, pre-pregnancy routine Cervical, to avoid multiple flow and induced abortions,master of pregnancy-related factors and premature rupture of membranes treatment, if there is dystocia occur, should be a timely manner in order to reduce neonatal morbidity and mortality.
[Key words] Preterm birth;Premature rupture of membranes;Causes;Pregnancy;Outcome
胎膜在临产前破裂称胎膜早破,俗称破水。妊娠满37周后胎膜早破率为10%;妊娠不满37周的胎膜早破率为2.0%~3.5%,发生率占分娩总数的6%~12%[1]145。胎膜早破常致早产、围生儿死亡、宫内及产后感染率升高。其原因多由:①胎位不正、头盆不称、骨盆狭窄等,使前羊膜囊承受压力过大,致羊膜破裂。②羊水过多、双胎等。③胎膜发育不良或有炎症致胎膜脆弱易破,妊娠晚期性交亦能促使破裂[2]。国内报道为2.7%~17.0%[1]。其围生儿发病率和病死率相当高,故应予以警惕。本文对134例早产合并胎膜早破产妇进行回顾性分析如下:
1 资料与方法
1.1 一般资料
本文对2007年1月~2008年6月在本院住院不足月胎膜早破者168例资料进行分析,所有产妇妊娠28~36+6周,平均年龄26.2岁,均未合并其他疾病。其中,初产妇133例,经产妇35例;单胎162例,双胎6例。
1.2 治疗方法
孕周为28~33+6周:抑制宫缩、促胎肺成熟、抗生素预防感染、能量合剂促进胎儿生长,尽量延长孕周至34以上。孕周为34~35+6周:抑制宫缩、促胎肺成熟、抗生素预防感染,待其自然分娩或选择缩宫素引产或选择剖宫产。孕周 36周:不建议保胎治疗,待其自然分娩或选择缩宫素引产或选择剖宫产。
2 结果
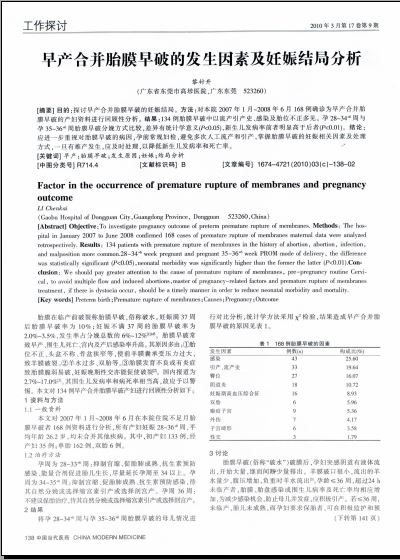
将孕28~34+6周与孕35~36+6周胎膜早破的母儿情况进行对比分析,统计学方法采用χ2检验,结果造成早产合并胎膜早破的原因见表1。
3 讨论
胎膜早破(俗称“破水”)破膜后,孕妇突感阴道有液体流出,开始大量,继而间断少量排出。羊膜破口很小,流出的羊水量少,腹压增加,负重时羊水流出[3]。孕龄≤36周,超过24 h未临产者,胎膜、胎盘感染或围生儿病率及死亡率均相应增加,为减少感染机会,防止母儿并发症,应积极引产 ......
您现在查看是摘要介绍页,详见PDF附件(1262KB,2页)。